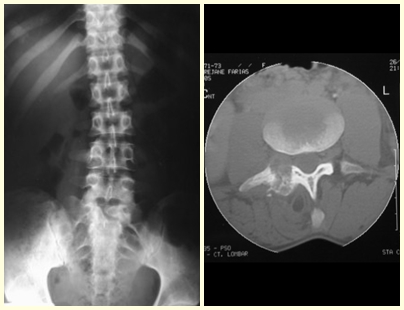
The vertebrae are also affected by this injury, including the sacrum. In the pelvis, the iliopubic branch is most frequently affected. They can mimic joint symptoms when they reach the epiphysis. Compromise in the spine can cause compressive neurological symptoms, although in most cases it affects the posterior structures.
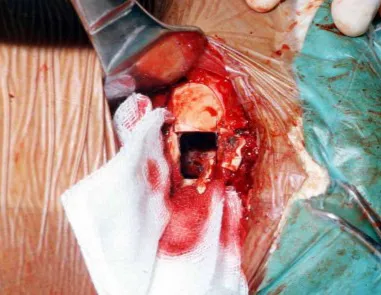
The treatment of choice has been marginal resection or intra-lesional curettage, followed by filling the cavity with an autologous or homologous graft, when necessary. The cavity can also be filled with methylmethacrylate, although our preference is to use an autologous graft when possible, as it is a benign lesion. Some authors associate intralesional adjuvant treatment with the application of phenol, electrothermia or cryotherapy. In classic aneurysmal bone cysts, I do not see the point of this therapy, which, however, should be applied when the surgeon finds a “suspicious” area that was not detected on imaging. If the aforementioned benign tumors are involved, which may be accompanied by areas of aneurysmal bone cyst, local adjuvant therapy will be beneficial.
Some bone segments such as the ends of the fibula, clavicle, rib, distal third of the ulna, proximal radius, etc. can be resected, without the need for reconstruction.
In other situations, we may need segmental reconstructions with free or even vascularized bone grafts or joint reconstructions with prostheses in advanced cases with major joint involvement. In the spine, after resection of the lesion, arthrodesis may be necessary to avoid instability.
Radiotherapy should be avoided due to the risk of malignancy, however it may be indicated for the evolutionary control of lesions in difficult to access locations, such as the cervical spine, for example, or other situations in which surgical re-intervention is not recommended.
Embolization as an isolated therapy is controversial. However, it can be used preoperatively to minimize bleeding during surgery. This practice is most used in cases of difficult access, although its effectiveness is not always achieved. Infiltration with calcitonin has been reported with satisfactory results in isolated cases.
Recurrence may occur, as the phenomenon that caused the cyst is unknown and we cannot guarantee that surgery repaired it. The recurrence rate can reach thirty percent of cases.
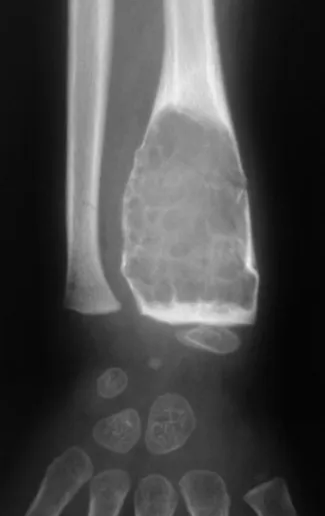
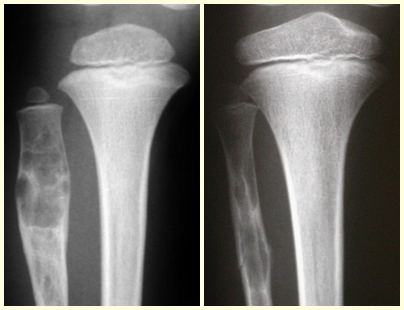
Simple Bone Cyst –
A simple bone cyst is a pseudo-tumor lesion that can occur in any part of the skeleton and most frequently presents with fracture (figures 59 to 64).