Pseudotumor Lesions – Simple Bone Cyst, Aneurysmal Cyst and Non-Ossifying Fibroma:
As for pseudo-neoplastic lesions , the one that most frequently causes fractures is the aneurysmal bone cyst . This process, of unknown etiology, which does not have a cystic appearance and much less is vascular in nature, is known as the benign lesion that has the most aggressive behavior, often simulating malignant neoplasms.
Other pseudo-neoplastic lesions that can fracture are the simple bone cyst of metaphyseal location, when in a bone with greater load such as the femur and tibia, it is prone to fracture. Non-ossifying fibroma , an evolution of the cortical metaphyseal fibrous defect, can also fracture due to its progressive increase in volume, when located in the metaphysis of the femur or tibia.
It is not uncommon for simple or complex bone fractures to hide pathological changes and may result in inadequate orthopedic treatment.
To treat pathological bone fractures, it is necessary to study the entire context that surrounds them. Bone fractures must always be analyzed under multidisciplinary aspects, which take into account the history, age group of the patients, clinical aspects, images, laboratory tests and anatomopathological examination. The joint multidisciplinary study of these data is essential for the diagnosis and management of each case. With the correct diagnosis, the orthopedist will define the treatment. Following what is described in this chapter:
Bone Dysplasias:
1 – Osteopsatirosis or Osteogenesis imperfecta.
Treatment : Clinical: The use of bisphosphonates is currently used.
Orthopedic: intramedullary osteosyntheses to support aligned growth, with telescoped rods, associated or not with osteotomies to correct deformities.
2 – Osteopetrosis
Treatment : Clinical: Prevention of deformities
Orthopedic: osteosynthesis of fractures
3 – Fibrous dysplasia, mono or polyostotic,
Treatment : Clinical: The use of bisphosphonates may have an effect.
Orthopedic: osteosynthesis
Metabolic Changes:
1 – Osteoporosis
Treatment : Clinical: prevention of fractures, avoid caffeine, walking. The use of bisphosphonates may be indicated.
Orthopedic: osteosynthesis of fractures
2 – Osteomalacia and rickets
Treatment : Clinical: Correction of homeostasis, vitamin D, prevention of deformities.
Orthopedic: osteosynthesis of fractures.
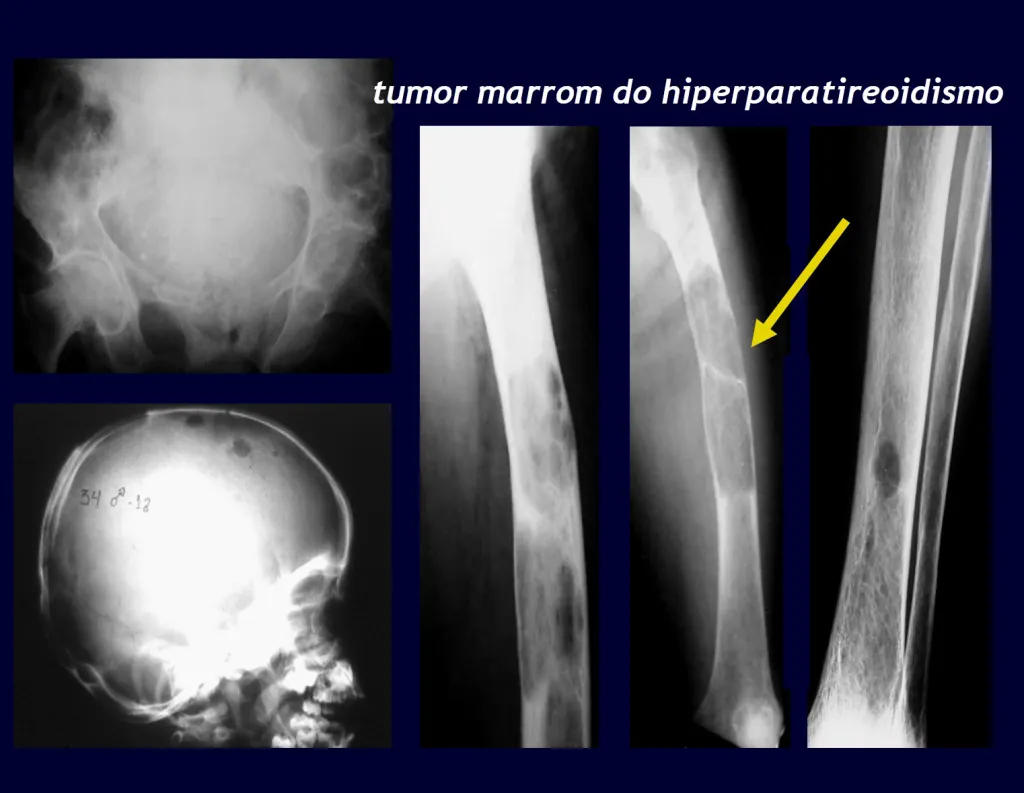
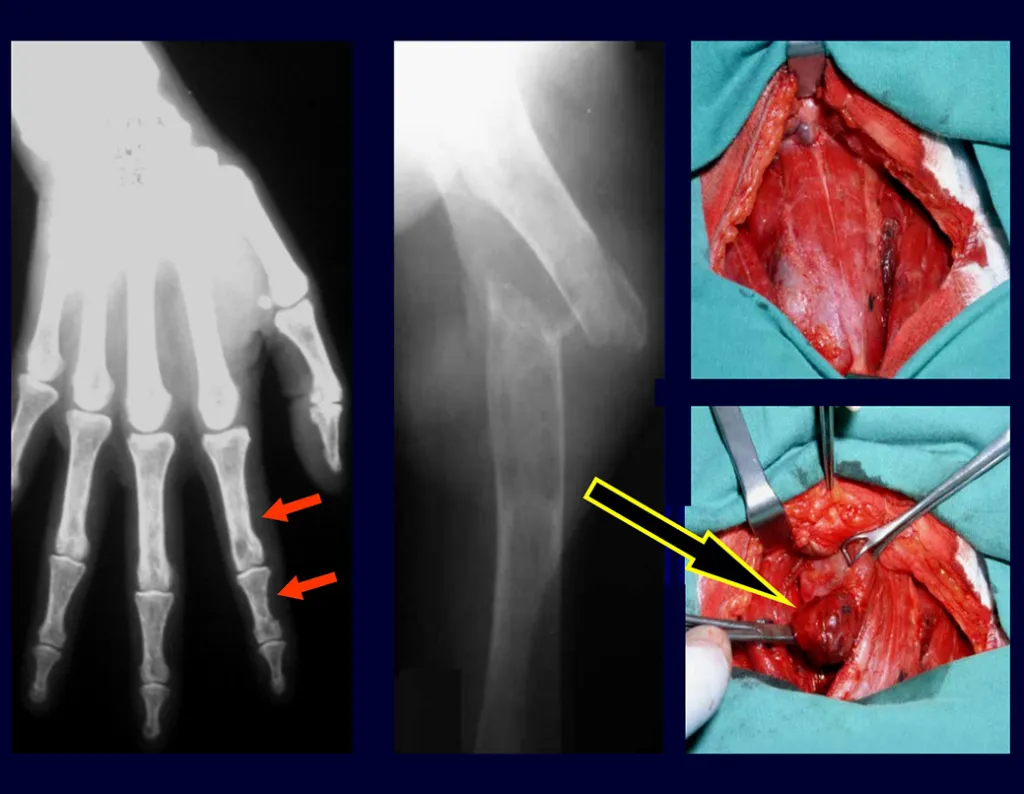
3 – Hyperparathyroidism
Treatment : Clinical: resection of the parathyroid tumor and compensation of the metabolic condition, taking into account the marked hypocalcemia that occurs after surgery, as the bone tissue begins to quickly compensate for the existing bone demineralization. Protein supply is essential for the creation of the bone matrix.
Orthopedic: osteosynthesis of fractures, which heal quickly, as the bone is starved for calcium.
Degenerative Diseases:
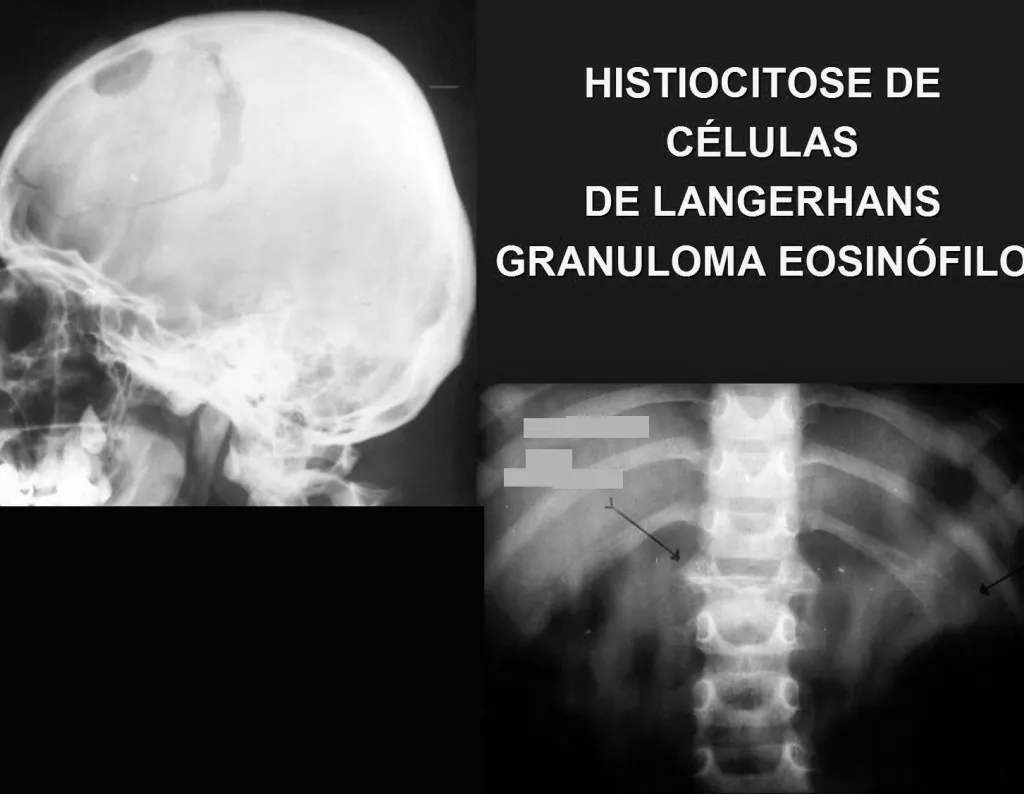
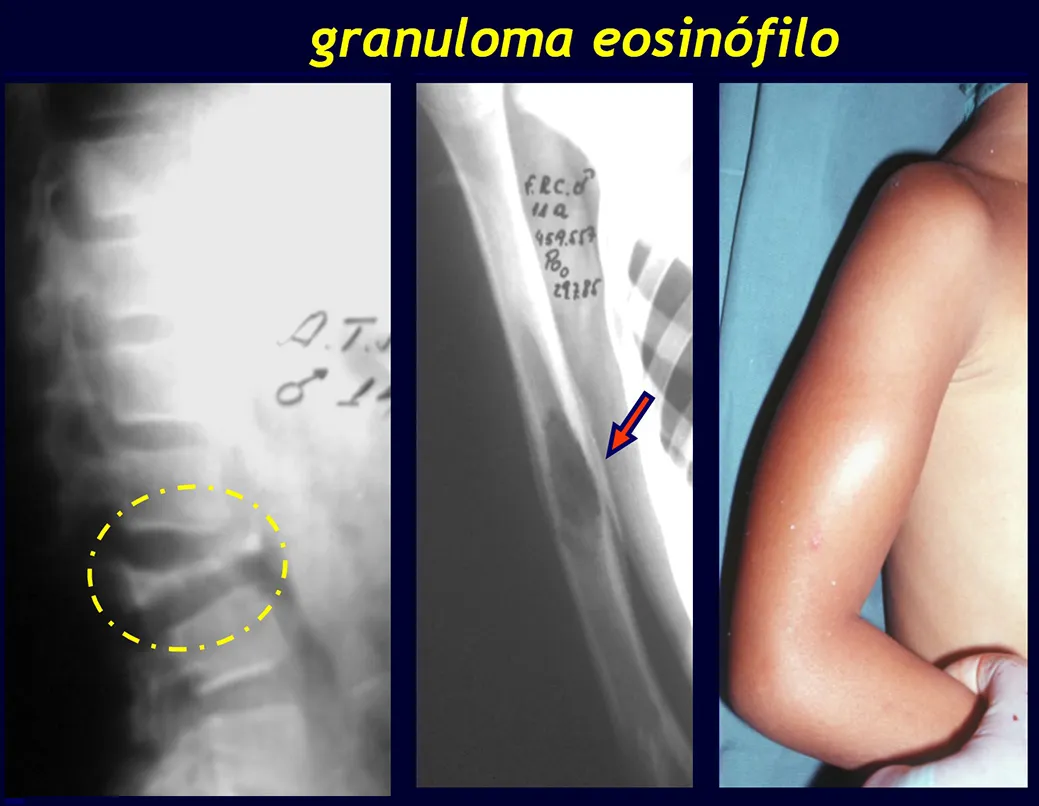
1 – Eosinophilic granuloma
Treatment : Clinical: corticosteroid therapy
Orthopedic: curettage of the bone lesion. In Calvé’s flat vertebra, the wedging fracture itself leads to healing of the process. In children and adolescents, the vertebral body spontaneously grows, correcting the deformity.
2 – Gaucher disease
Treatment : Clinical:
Orthopedic:
Circulatory disorders:
1 – Paget’s disease
Treatment : Clinical: Bisphosphonates and anti-inflammatories.
Orthopedic: osteosynthesis of fractures
2 – In blood dyscrasias
Treatment : Clinical:
Orthopedic:
Inflammations:
1 – Hematogenous osteomyelitis
Treatment : Clinical: antibiotic therapy
Orthopedic: drainage of abscesses, removal of bone sequestra and stabilization of fractures.
2 – Tuberculosis
Treatment : Clinical: triple regimen for tuberculosis.
Orthopedic: cleaning of caseous abscesses and immobilization, with arthrodesis of the affected joints and osteosynthesis of fractures often being indicated.
3 – South American Blastomycosis , whose agent is paracoccidioidis brasiliensis and
Treatment : Clinical: specific drug treatment for ringworm
Orthopedic: surgical cleaning and specific care for each case.
4 – Echinococcosis, in the form of a hydatid cyst, must be treated surgically.
Neoplasms:
1 – Benign primitives : Orthopedic treatment can include intralesional curettage, local adjuvant, reconstruction with osteosynthesis and autologous graft or methyl methacrylate.
2 – Malignant Primitives : May require neoplasia-oriented chemotherapy treatment and surgical treatment of resection and reconstruction with endoprostheses or biological reconstruction, if possible, or ablative surgery.
3 – Secondary to metastases : Restoring function is essential for the patient’s quality of life. The treatment option for these fractures requires some consideration to make the appropriate choice for each patient. Some of them are subjective, as we have to assume the patient’s likely survival time, clinical possibility that they will fully recover their functions, ability to withstand anesthesia, etc.
We seek to support our decisions on the following parameters:
- Is the injury to the upper limb, lower limb, pelvic girdle or spine?
- Is the injury single or are there multiple injuries?
- Has the fracture already occurred or is there a risk of fracture?
- If no fracture occurred, is 1/3 of the bone’s circumference already compromised? Does the injury cover a long area?
- Did the patient walk before the fracture, did he have normal motor function?
- How long has the patient been treated for the primary disease?
- Are you currently receiving chemotherapy treatment?
- What is this patient’s temporal prognosis?
- What co-morbidities do you have in addition to the neoplasm?
- The type of primary neoplasm responds to radiotherapy
The analysis of these issues will allow a therapeutic decision to be made that assists the patient in recovering their motor function, in line with the treatment of their underlying disease.
Patients with myeloma have a high rate of postoperative infections and usually benefit from local radiotherapy, especially in lesions of the thoracic spine or upper limb, in the first years of the disease. After a few years, when the disease becomes refractory to chemotherapy or bone marrow transplantation, even surgical options are limited due to the intensity of bone involvement.
This case in figures 8 to 12 exemplifies a patient with multiple myeloma, presenting an extensive lesion in the proximal half of the right humerus. Despite being myeloma, which responds well to chemotherapy and radiotherapy and even in the upper limb, there is an indication for resection of the lesion and reconstruction with a non-conventional endoprosthesis due to the destruction of the anatomy and providing prompt restoration of function.